Published in the Hampshire Gazette Feb. 23, 2022. This open letter was co-authored with Seth Cable, Summer Cable, Michael Stein and Susan Voss, and was also signed by 216 other people that live and work in Hampshire County, listed at the end of this letter. For further information on Covid safety in schools, please see the Urgency of Equity toolkit.
An opinion column published in the Hampshire Gazette on Feb. 17 2022 claims that “even if at one point in the pandemic it was possible to make a reasonable argument for the masking of children in school, that is no longer the case”. We disagree, since the following provides what we take to be a clearly reasonable basis for deciding to continue the school mask mandates until the levels of community transmission subside to a much lower level. We offer this as a statement of views that we believe are widespread, but are usually not made as vocally as those of the opponents of mask mandates and other public health measures.
1. It is reasonable to minimize spread in our community by using school masking. Our children interact with other members of the community, some of whom are relatively vulnerable to the effects of Covid-19 infection. By slowing spread in our schools, we are also slowing spread in our communities. The authors of the opinion column claim that “[t]here are no credible scientific data indicating that masking of children in schools has limited the spread of COVID-19”. They do not say why they do not consider the data presented by the CDC or other data to be credible. It is possible that they consider only data from randomized controlled trials (RCTs) to be credible, since they say in the next sentence that “[n]o randomized controlled trials of mandatory school masking have been carried out”. The CDC and other experts clearly consider sources of evidence other than RCTs to be useful, and it is not difficult to imagine why no RCTs have been run on school masking. For example, Institutional Review Boards may well balk at approving a study with a control group of unmasked students in a community with high transmission.
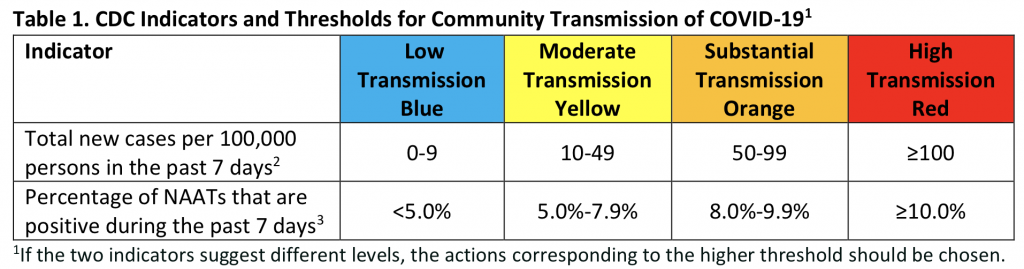
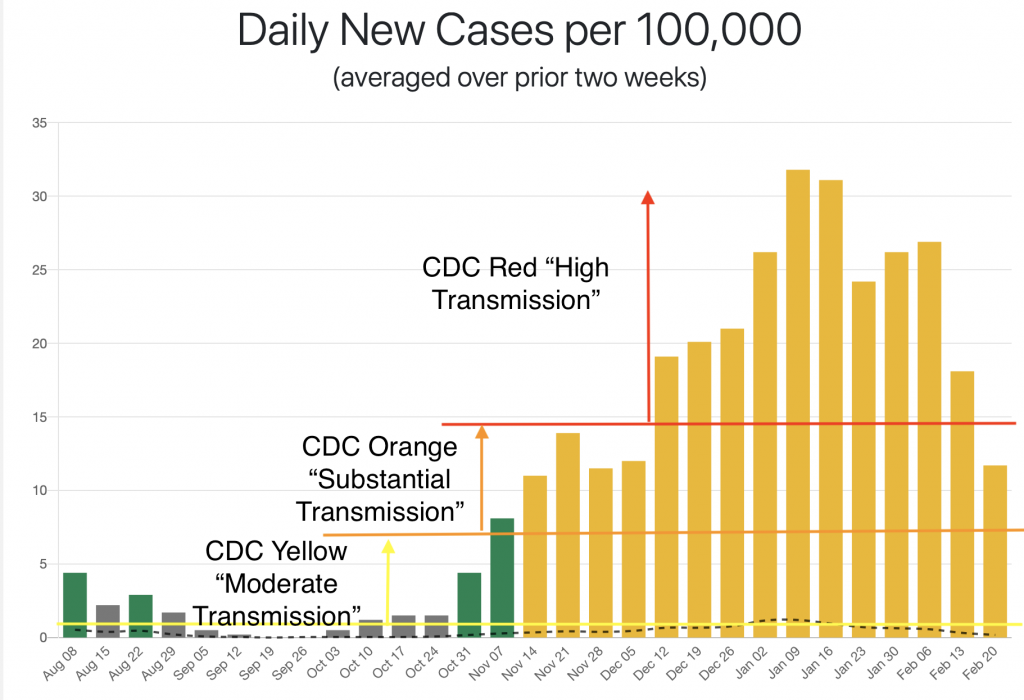
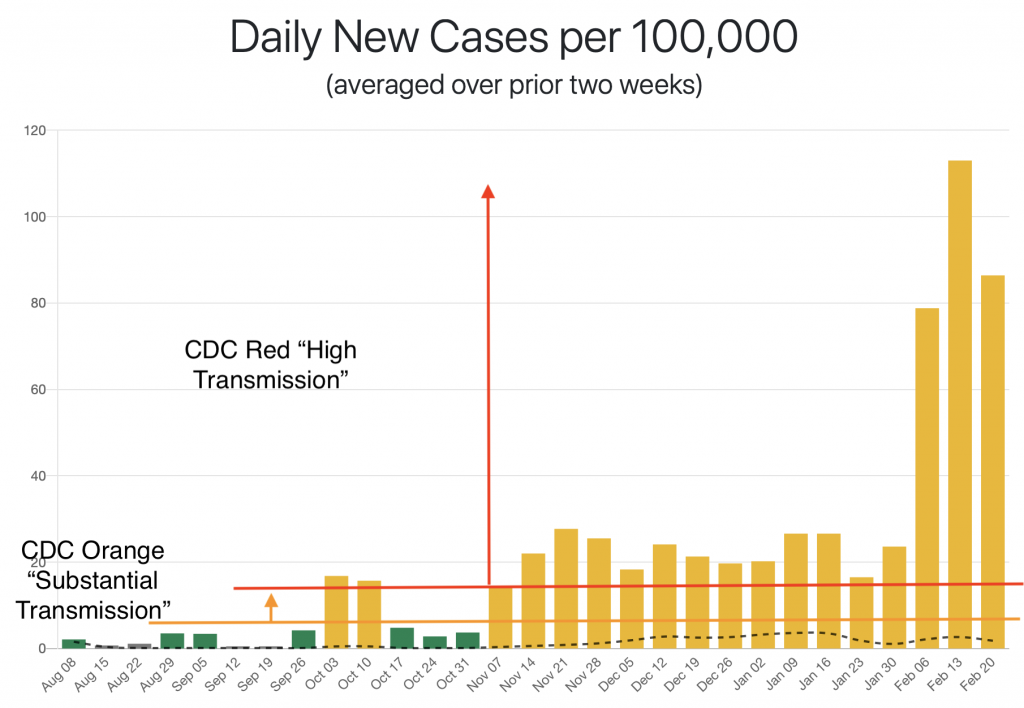
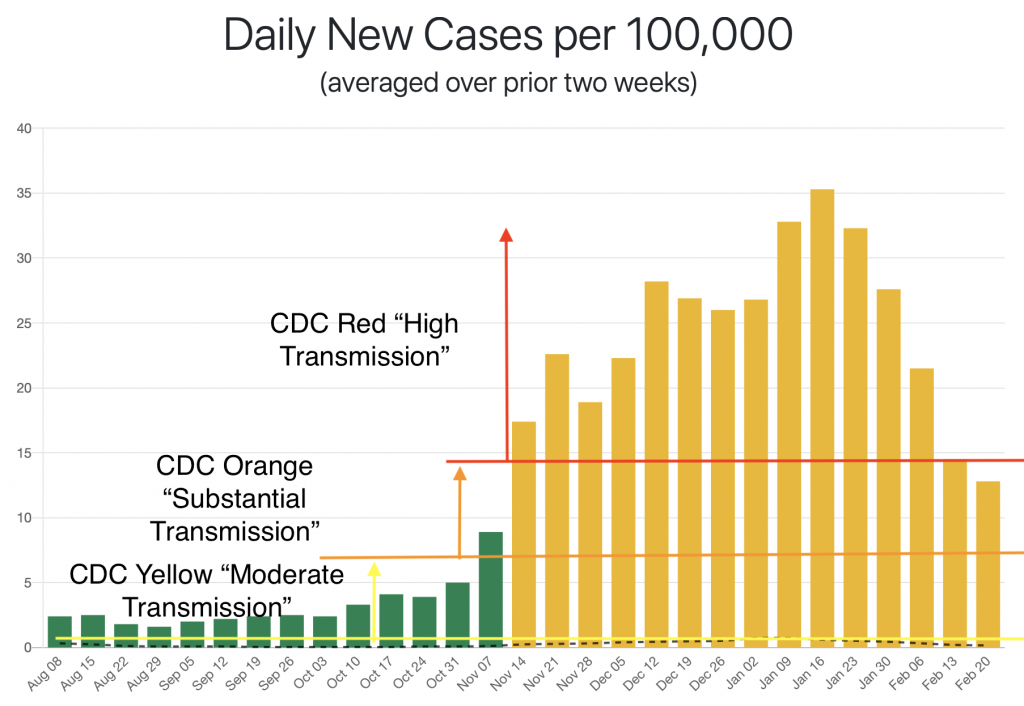
2. It is reasonable to characterize the current local level of community transmission as high, and the risk to community health of that transmission as high as well. According to Mass-DPH data, there were 680 new cases in Hampshire County the week ending Feb. 17, which translates to a per capita rate that is over 4 times the CDC’s bar for “high transmission”, and over 8 times the bar for indoor mask wearing. Many of those cases are likely from an outbreak at UMass Amherst, which reported 456 cases in the week ending Feb. 15th. The future impact to the broader community of that outbreak is unknown. The Mass-DPH reports 37 Covid-19 deaths in the last 28 days in Hampshire County, which can reasonably be taken to indicate a high community health risk.
3. It is reasonable to minimize Covid-19 infections in our children. While most children recover quickly from Covid-19 and have mild symptoms, some wind up in hospital, and some die. That the proportion of deaths is lower than in adults, or that the number is lower than child deaths from some other cause, does not make it any less desirable to avoid those deaths. In addition, the long-term effects of these infections is unknown. There are clearly long-term effects of Covid-19 infections in general. We can only hope that childhood infections with Omicron, especially in vaccinated children, will have fewer long-term effects.
4. Mandates maximize the protection of each individual. If everyone in a room wears a mask, the amount of airborne virus is minimized, maximizing the protection for everyone. It is a less effective protection for an individual if others are maskless. This is especially true if that individual does not have the mask perfectly fitted, or occasionally takes it off to eat or drink, circumstances that seem common in a school. Wearing a mask is not just about protecting oneself, it is also for the protection of the community, including its most vulnerable members. For example, universal masking allows children who are immune compromised or otherwise at high risk for severe disease and children who have family members who are immune compromised to attend school when it would otherwise be unsafe to do so.
5. It is reasonable to decide that real or potential negative effects of masking are outweighed by their positive benefits in minimizing Covid-19 infections. There seems to be no good evidence of negative effects of masking on child development. It is quite possible that speakers of non-mainstream varieties of English (e.g. second language speakers) may be more impacted than others by mask wearing. Real and potential negative effects should be taken into account in any decision about a mask mandate, and attempts should be made to address them when masking is in effect. But it may well be that the benefits of masks outweigh any risks.
Signed by:
Joe Pater, Northampton resident and Professor of Linguistics, UMass Amherst
Summer Cable, Northampton resident
Seth Cable, Florence resident and UMass Faculty
Susan Voss, Northampton resident and Professor of Engineering, Smith College
Michael Stein, Northampton Resident, Ward 4 School Committee Member
Jennifer Ritz Sullivan, COVIDJustice Leader for Massachusetts with Marked By COVID Goshen
Suzanne Theberge MPH, Northampton
Tom Roeper, Amherst
Naomi Gerstel, Professor emerita UMass, resident Northampton
Rene Theberge, Retired Public Health Worker, Florence
Neil Kudler MD, Physician
Kirsten Leng, Resident of Northampton, Associate Professor, Women, Gender, Sexuality Studies, University of Massachusetts Amherst
Jean Potter, Doula, Northampton
Frazer Ward, Northampton
Erica Kates, Florence, MA
Thomas Wartenberg, Professor of Philosophy, Emeritus, Mount Holyoke College
Jen Davis, Northampton
Lou Davis, Financial Planner and Advisor, Northampton
Wenona Rymond-Richmond, Northampton
Eric Poehler, Northampton
Karen Foster, Ward 2 City Councilor
Erin Kates, Resident of Florence
Sarah Metcalf, writer, Northampton resident
Christopher Pye, teacher, Northampton resident
Andrew Kennard, Postdoctoral Fellow, UMass Amherst. Amherst resident
Tom Riddell, Northampton
Beth Adel, Teacher and resident of Northampton
Elliot Fratkin, Professor Emeritus Smith College. Northampton
Sally Popper, Retired, Northampton
Robert Buscher, Northampton
Laura Briggs, Professor, University of Massachusetts and Northampton resident
Maureen Flannery, Northampton
Steven Goode, Northampton
Christopher Golden, parent and NOAA software engineer, Northampton
Hedy Rose, retired educator, Northampton resident
Norma Akamatsu, Social Worker, Psychotherapist, Northampton
Ian Goodman, MD, Pediatrician and Northampton Resident
Angela Silvia, CT technologist, Northampton, MA
Meg Robbins, Resident, Northampton, MA
Traci Olsen, Northampton
Jennifer L. Nye, Northampton resident and UMass Amherst faculty member (History)
Anisa Schardl, Northampton Public Schools teacher and parent
Janet Gross, Retired
Nicolas Gross, Retired
Matthew Hine, Service Engineer (Aerospace), Northampton
John Selfridge, public school teacher, Northampton
Sara Lennox, Northampton
Jill de Villiers, Professor, Smith College, Northampton resident
Daniel Cannity, Northampton Resident
Rachel Merrell, Teacher
Cora Fernandez Anderson, Assistant Professor at Mount Holyoke College, Amherst resident
Melinda Buckwalter, Williamsburg
Emily Hamilton, Professor of history of science/medicine
Taylor Flynn, Parent & retired professor, Northampton MA
Deborah Keisch, Florence
Adele Franks, Public health physician, retired
Young Min Moon, Professor, UMass Amherst
Jude Almeida, School-Based Social Worker, Northampton resident
Karin Baker, Teacher, Northampton
Meghan Armstrong-Abrami, Associate Professor of Hispanic Linguistics, Northampton resident
Lynn Posner Rice, Northampton
Justin Pizzoferrato, Father/self employed
Greg Lewis, Public Health Emergency Planner, Northampton
Alyssa Lovell, school-based OTR/L
Kim Gerould, Northampton
Omar Dahi, College professor
Kai Simon, Northampton
Andrea Ayvazian, Pastor, Northampton resident
Jennifer Fronc, UMass Faculty; Northampton resident
Graciela Monteagudo, Senior Lecturer, UMass Amherst, Amherst Resident
Roberta Issler, Retired teacher
Cathy McNally consultant, Northampton
Rachel Wysoker, Northampton
T. Stephen Jones, MD, MPH retired public health physician
Alison Morse, Educator
Cory Ellen Gatrall, Registered Nurse
John McNally, Attorney and grandparent, Northampton
Jeff Napolitano, Northampton, MA
Rebecca Busansky, Northampton
Rachel Yox, Amherst
Judd Gledhill, Director IT
Meg Bogdan, Parent of Northampton Public School Students
Roz Chapman, Northampton
Lisa Weremeichik, Northampton
Charles Dumont, MD MS Pulmonary and Critical Care physician
Tara Dumont, MD Physician
Rebecca Burwell, Professor
Karen Sullivan, College staff, Northampton
Victoria Dixon, Disabilities Advocate, Amherst
Leah Greenberger, veterinarian, Belchertown MA
Annie Salsich, Self-employed
Gabriel Phipps, Adjunct Professor
Karen Hodges, Florence
Katherine Fabel, DUA and Lecturer, UMass Amherst, Florence MA
Nykole Roche, Northampton resident w/3 kids in NPS
Garrett Warren, Amherst
Annabelle Link, Northampton
Capella Sherwood, Music teacher/ Northampton
Bertha Thorman, Northampton
Neha Kennard, Amherst
Kelly Link, Writer
Lesley Yalen, Florence, MA
David Arnold, UMass Professor of Psychological and Brain Sciences
Kristen Elde, Leeds
Lisa Harvey, Professor of Psychological & Brain Sciences at UMass, Resident of Amherst
Michael Becker, Hadley resident and UMass Faculty
Henry Rosenberg, Northampton
Andrew Gorry, Staff, UMass Amherst
Eddie (Erin) Gorry, UMass Staff, Resident of Florence, MA
Leeba Morse, Grant Writer
Jonathan Knapp, Northampton Public Schools educator
Alexis Callender, Works as faculty in Northampton, Lives in Easthampton
Megan Paik, Northampton
Mary Hoyer, Amherst resident and retired Hartford Public Schools teacher
Terianne Falcone, Writer / teacher
David Ball, Northampton
Renee Spring, Amherst Psychotherapist
Therese Kim, Social Worker
Anand Soorneedi, Amherst
Dorcas Grigg-Saito, Northampton, retired Community Health Center CEO
Erica Deighton, Retired educator, Amherst resident.
Steve Waksman, Elsie Irwin Sweeney Professor of Music, Smith College
Cornelia Daniel, Retired in Amherst
Christine Clark, Dental Hygienist
Wendy Sutter, Amherst resident
Lijah Joyce, Amherst
Patricia Maynard, Retired teacher. Northampton resident
Heather Brown, Educator, Northampton
Marissa Elkins, Attorney/City Councilor
Mary Savarese, Retired Teacher
Peggy Matthews-Nilsen, Amherst (Psychotherapist, Retired)
Julia Frisby, Hatfield MA
Karen Osborn, Anherst
Lisa Moos, Physical Therapist Assistant
Patricia Duffy, Leverett
Barbara Palangi, Retired
Elizabeth Jimenez, Northampton
Sandy Oldershaw, South Hadley
Tania Menz, Hatfield Resident, Hadley Family Physician
Kimberly Schlichting, resident of Hadley, teacher in Northampton
Elizabeth Hallstrom, resident of Amherst
Kasey Mimitz, Youth services coordinator
Scarlett Mimitz, Student
Nora Mimitz, Student
Emily Kawano, Non-profit Co-director
Jalen Michals Levy, EMT-B
Andrea Gaus, Farmer, Hatfield
Melanie Miller, Northampton
Daniel and Angela Dee Amherst
Sandra Torrence, Teacher
Michelle Trim, Faculty at UMass Amherst/ South Hadley
Roberta Pato, Retired teacher, Northampton
Barbara Partee, Amherst resident and Professor Emerita, UMass Amherst
Norma Brunelle, Retired
Raymond R. Brunelle, Retired
Mark Brunelle, Laborer
Joanne Brunelle, Dental Assistant
Barbara Cooper, Retired teacher/librarian
Toni Brown, Hatfield
Faruk Akkus, Faculty at UMass Amherst
Felice Swados, South Hadley
Victoria Rosen, Northampton
Felice Swados, South Hadley
Victoria Rosen, Northampton
Jon Wynn, UMass Amherst, Associate Professor, Northampton Resident
Zelia Almeida, RN Pediatric ICU/ Belchertown
Marci Linker, Occupational Therapist and Northampton resident
Lindsay Whittier-Liu, Northampton
Sarah Wolfe, Northampton paralegal, resident of Belchertown
Jean Fay, Amherst educator
Lance Hodes, Pelham
Alex Robinson, Amherst
Barry Seth, Student in Amherst
Oliver Dubon, Amherst
Basil Perkins, College Student
Ivonne Vidal, Belchertown, Attorney
Tina Cornell, Florence
Judith Trickey retired
Lisa Packard, Amherst
Bennett Lyons, Amherst, MA
Kate Matt, Shutesbury
Anne Hazzard, Amherst
Isolda Ortega-Bustamante, fundraiser; Amherst
Maureen Vezina, Belchertown
Evelyn Trier, Mount Holyoke College Admission/ Amherst resident & parent
Katherine Kraft, retired, Amherst
Marshall Cohen, retired, Amherst
Monroe Rabin, retired
George Collison, retired prof
Emilie Hamilton, Amherst
Stefan Gonick, Belchertown
John Hondrogen, retired and still masking in Pelham
David Gross, Pelham
Lili Kim, Amherst
Susan Watkins, Shutesbury
Amelia Vetter, Student, Amherst
Dan Levine, Business Owner
Theresa Ryan, Realtor
Jenny Miller Sechler, Psychotherapist, Northampton
Matthew Levin, retired pre-school/k teacher (Northampton)Hatfield (residence)
Robert Jackson, Amherst
Amy Dopp, Easthampton
Keri Heitner, Amherst
Anita Sarro, Retired Nurse-Attorney
Amy Hirsch, Psychologist
Emily Case, Amherst parent, Hatfield educator
Michelle McBride, UMASS Employee in Linguistics Department
Kimberly Stillwell, Speech Language Pathologist, Northampton
Delia Martinez, Retired teacher-keep masks in schools
Amy Martyn, Florence
Rebecca Leopold,Northampton, retired Amherst-Pelham HS teacher
Alicia Lopez, Teacher, Amherst
Sharon Moulton, Northampton
Louis Faassen, Architect
Scott Billups, Shutesbury
Jacqueline A. Faison, Pelham
Seth Lepore, Arts and Small Business Consultant, Easthampton, MA
Rachel Brod, Northampton
Stephanie and David Kraft, Retired
Jack Howe-Janssen, Florence
Annette Gates Teacher, Crocker Farm Elementary